








Laryngoscopes, as precision medical endoscopic components, require injection molds that directly impact biocompatibility, dimensional accuracy, and clinical safety. Manufacturing must strictly adhere to medical-grade injection molding standards, with no compromise in design, material selection, or process control.
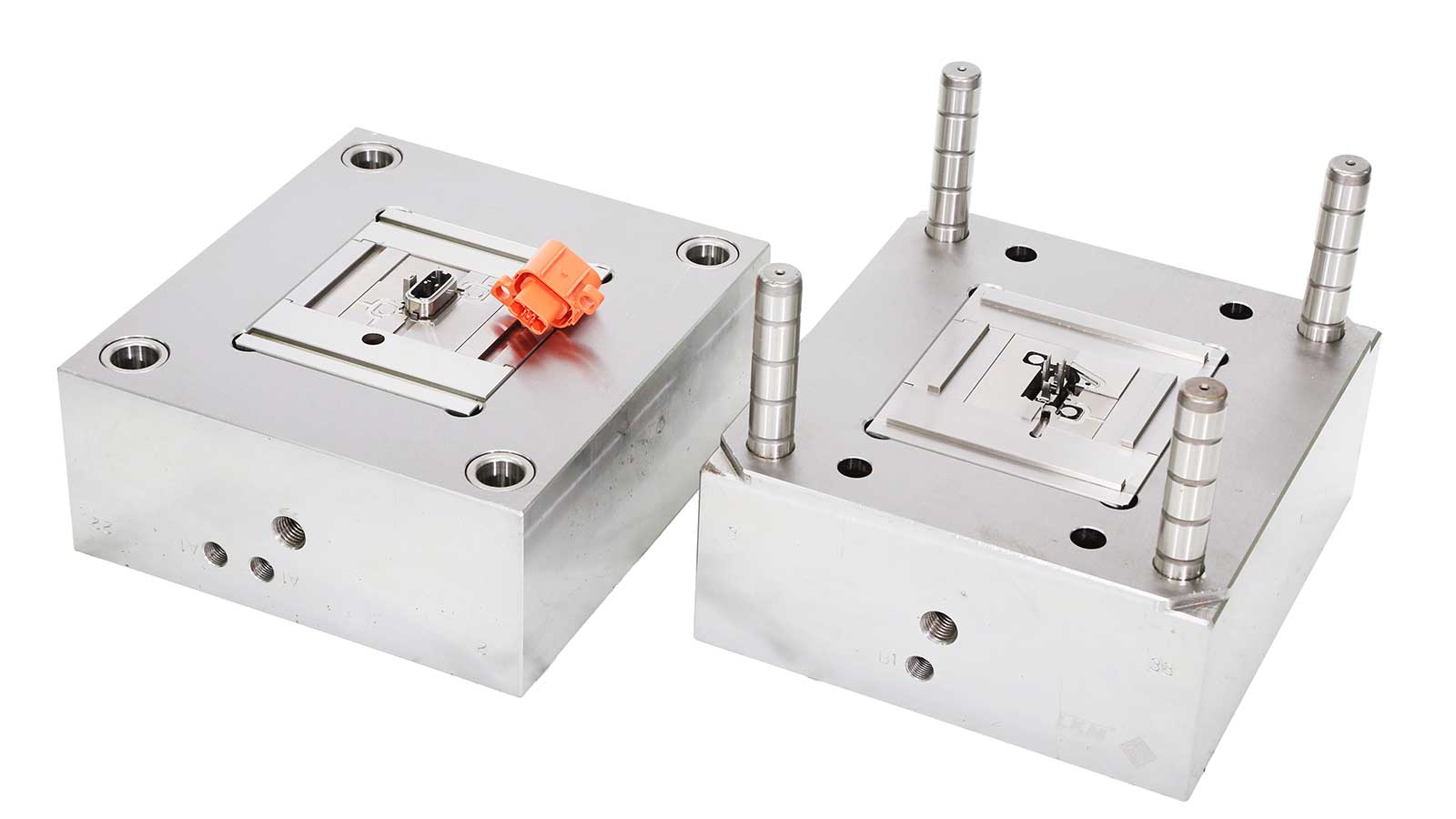
Structural Design Considerations
Due to the laryngoscope’s small size and thin walls, mold design must prioritize complete cavity filling. Gates should be designed as pin-point submarine types, positioned in non-visible areas to avoid post-molding marks that compromise aesthetics and cleanability. Parting lines must avoid critical functional surfaces to minimize seam interference with surface finish. Ejection draft angles should be ≥1.5°, with external surface drafts exceeding internal drafts in deep-cavity structures to prevent core shift and wall thickness variation. Rib thickness must not exceed 70% of the nominal wall thickness to prevent sink marks. All radii must be ≥0.2mm to reduce stress concentration and extend mold life.
Material and Surface Treatment
Cavities and cores must be fabricated from high-polish stainless steel (e.g., S136 or H13 pre-hardened steel), with surface roughness controlled to Ra≤0.8μm, and critical areas achieving Ra≤0.4μm to meet medical-grade cleanliness standards. Mold bases should be constructed from corrosion-resistant steel to withstand prolonged exposure to disinfectants and cleaning agents. All coolant channels, ejector pin bores, and insert joints must be designed without dead zones to eliminate material accumulation and bacterial growth.
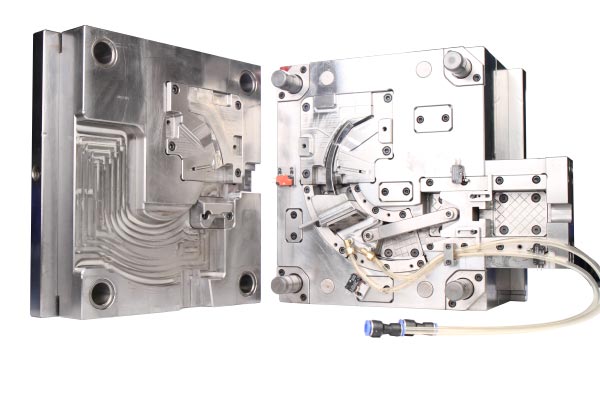
Cooling and Venting Systems
Given typical wall thicknesses under 1mm, cooling efficiency directly affects cycle time and warpage control. Spiral through-core cooling channels are recommended to ensure coolant contact with the forming surface, maximizing heat transfer. Independent temperature control of moving and fixed mold halves is essential, with temperature differentials maintained within ±2°C to prevent barrel distortion. Venting grooves must be located at the melt flow end, with depths ≤0.02mm and widths of 3–5mm to prevent trapped air from causing burns or weld lines.
Process Control and Regulatory Compliance
Production must occur in a cleanroom environment compliant with ISO 13485 quality management systems, ideally at a Class 100,000 level. Injection parameters must be validated through PQ (Performance Qualification): barrel temperature fluctuations ≤±3°C, injection pressure between 80–120MPa, and holding time precisely calibrated to wall thickness. Recycled or non-medical-grade resins are strictly prohibited; all materials must be accompanied by a Certificate of Analysis (CoA) and USP Class VI biocompatibility certification.
Common Technical Challenges and Mitigation Strategies
Flash typically arises from parting line gaps >0.03mm or insufficient clamping force. Prevention requires high-rigidity mold frames and regular flatness inspections. Incomplete filling due to uneven melt flow can be resolved through mold flow analysis to optimize gate location and runner cross-section. Silver streaks on surfaces are commonly caused by moisture in the resin; pre-drying to moisture content <0.02% is mandatory. Standardized cleaning procedures using non-linting cloths and medical-grade solvents must be implemented to prevent contamination.
FAQ
Q1: Can standard plastic mold materials be used for laryngoscope molds?
No. Standard mold steels are susceptible to corrosion from disinfectants, potentially releasing metal ions that violate medical biocompatibility requirements. Only mirror-polished stainless steel must be used to ensure long-term resistance to corrosion and leaching.
Q2: Why is surface finish so critical for laryngoscope components?
Laryngoscopes contact human mucosal tissue; surface roughness exceeding Ra>0.8μm can harbor bacteria and promote biofilm formation, increasing infection risk. Surfaces above this threshold cannot be reliably sterilized or cleaned, violating ISO 13485 requirements for reusable medical devices.
Q3: What is the typical mold lifespan, and how can it be extended?
Under proper operation, high-quality laryngoscope molds can reliably produce over 500,000 cycles. Extending service life requires regular cavity polishing, precise temperature control to prevent resin degradation, use of rust-inhibiting coolant, and avoidance of overpressure operation.
Q4: Is a sterile mold required?
The mold itself does not need to be sterile, but it must be “dust-free and contamination-free.” Production must occur in a cleanroom, and mold design must allow for effective sterilization via steam autoclaving or ethylene oxide, with no hidden crevices where debris can accumulate.
Q5: How is flash detected and prevented?
Flash can be detected using high-magnification microscopy or coordinate measuring machines; any thickness >0.05mm is considered defective. Prevention hinges on achieving >95% contact area across the parting line and employing closed-loop pressure control systems to stabilize injection parameters.
